
“Putting those with Lived & Living Experience front and centre”
Introduction
Finding the starting point to write this short blog about developing Peer-to-Peer naloxone training and supply programs has been really difficult for me. If I’m honest, I have felt totally paralysed and stuck for words, which for any who know me will also know words (and too many of them) are generally my thing.
Anyway, let’s do this!! My name is George Charlton, I’m an ex-drug user, I’ve spent many years battling addiction, feeling the pain of the war on drugs, well actually the war on people like me who use drugs! I was a poly drug user meaning that my drug of choice was “more”, more of anything I could get my hands on!
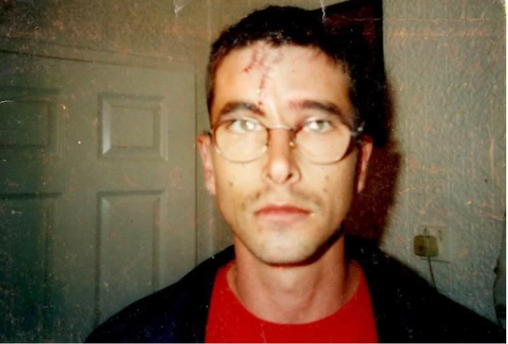
I committed crimes to fund my drug habit, my crimes put me in jail, seen me written off by society, written off by my friends and also written off by myself. I hurt my family and I hurt myself. I had countless opiate overdoses, seeing my life being saved in hospitals across the north East of England on countless occasions.
I have spent much time detained under the mental health act and long before I ever took a drug I was broken, owing to adverse childhood experiences and trauma which I experienced as a child. I never believed back then that my life was worth anything or that I was capable of achieving anything, but it was and I have!!
Taking drugs for me over the years was a means of medicating and treating my emotional pain and trauma, and for me back then, just like many hundreds of thousands of people right now across the UK impacted by addiction and trauma, I, like them was classed the scum of the earth, someone not to be trusted and someone who should most definitely know their place.
Over the past 20 years of working with people who use drugs I too have come to believe that in fact “Drug Users” should know their place and that place, I firmly believe, is front and centre and at the heart of every treatment system and service across the UK and this is what my blog today is all about.
I too have come to believe, that in fact “Drug Users” should know their place, and that place I firmly believe, is front and centre and at the heart of every treatment system and service across the UK
Putting people with lived and living experience at the heart of everything.
It Shouldn’t be this hard to save a life: But in some parts of the UK it can be
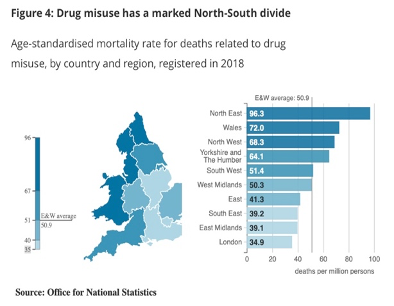
In October 2018 I tried to get a Naloxone kit from the local drug treatment service where I lived. During that time, Drug Related Deaths in the North East of England were again at an all-time high, where according to the ONS (2018) across England and Wales:
- There were 4,359 deaths related DRD’s in 2018, the highest number and the highest increase (16%) since numbers began in 1993.
- Since 2006, over half of all deaths involved an opiate. In 2018, a total of 2,208 DRD’s had an opiate mentioned on the death certificate.
- The North East where I lived, had a significantly higher rate of deaths relating to drug misuse than all other English regions.
During this time, I was working with people who were using drugs and felt I was not prepared to save a life in the event that someone overdosed around me. To be honest I had no idea what I would do other than phone 999, which incidentally is what you should do. However, I had heard about Naloxone and was told I would be able to get one without too much trouble. In reality, when it came to getting my hands on a Naloxone kit, it was a very different story.
I called the treatment provider who supplied Naloxone, once, twice, sent an email, more calls, I was told I would get a call back on countless occasions, the call never came. In the end, after 6 weeks of chasing on my part, I finally got to speak to a nurse who told me that even though they had responsibility for Naloxone Training, she would need to ask her boss if I could be trained and given a kit.
My email was again taken, and this time I did receive a reply….. the email reply said:
“we are very sorry George we cannot action your request”
That was it, nothing else, no explanation. My first thought was to go mad and start working my way up the organisation's management structure to say how angry and concerned I was that I could not get access to something I had been told should be extremely easy to get, however, instead, in that one moment, a thought came to me, “it shouldn’t be this hard to save a life” and I made a vow right there and then that I was going to do something about this myself, and this is where my journey with Naloxone began.
It should be noted that during the period 2017/18 findings from the Release ‘Finding a needle in a Haystack’ report suggested that Naloxone Supply, whilst showing some improvement from previous years was still limited across the England:
“Of the 152 local authorities in England, 145 reported dispensing a total of 40,033 THN kits in community settings for an estimated 244,457 people using opiates. On this basis, the estimated national coverage of THN among people who use opiates in 2017/18 was 16 per cent, which suggests that the amount of THN given out across England in 2017/18 was limited”
To the service who made things so difficult for me, and whom out of professional courtesy shall remain nameless, I want to say thank you, thank you for not supplying me with Naloxone on the day I asked for it... If you had I may not have gone on to spend the last 2 years co-producing awesome peer led projects with some amazing people and providers all of whom want to put those with lived and living experiences at the heart of their projects.
What is naloxone? Naloxone is a wonder drug! trust me, I’m alive because of it!!
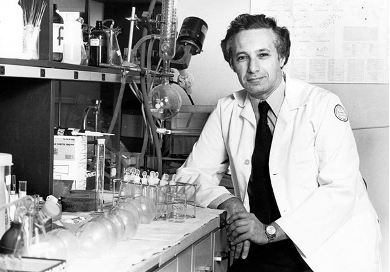
Widely heralded as the “antidote” to opioid overdoses, naloxone was first patented in New York in 1961 and discovered by a scientist called Dr Jack Fishman whilst exploring ways to treat constipation caused by chronic opioid use. Dr Fishman managed to synthesise the drug, but instead of making a laxative, he found the new molecule acted as an opioid antagonist, a compound that could aggressively outcompete other opioids in sticking to the brain’s receptors.
Naloxone works by blocking the opioid receptors to counteract the effects of opioid drugs such as heroin, methadone, fentanyl and morphine. The main life-threatening effect of these central nervous system depressant’s is that they can slow down and eventually stop a person from breathing, which is why Naloxone is so important. Naloxone blocks this effect and reverses the breathing difficulties experienced by a person in an Overdose situation. Naloxone itself has no psychoactive properties and has “no intoxicating effects or misuse potential”
According to EuroNpud’s Technical Briefing on Peer-to-Peer Naloxone Distribution:
“Naloxone can reverse the effects of overdose if administered within a short period following an opioid overdose. When administered intramuscularly the onset of action is between 2-4 minutes. The duration of the naloxone is up to 45 minutes. When someone accidentally overdoses and opioid drugs are involved, their breathing can be compromised, and this can lead to their death”
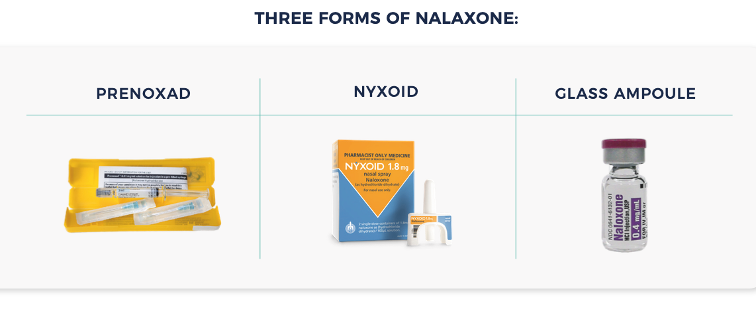
Naloxone is available in prefilled syringes with 5 x 0.4mg doses of naloxone (PRENOXAD) and the nasal form of naloxone now also has a European license (NYXOID). In many contexts around the world, naloxone is also available in a 0.4mg Glass Ampule.
Naloxone is not a new drug and has successfully been used in emergency medicine in hospitals and by medical staff and ambulance personnel across the globe since the 1970s to reverse the respiratory depression caused by opioid overdose. It is included in the World Health Organization’s list of essential medicines and within the WHO 2014 guidelines on ‘Community management of opioid overdose’ it is recommended that access to naloxone should include: “people likely to witness an overdose in their community, such as friends, family members, partners of people who use drugs, and social workers.”
Guidance from PHE in 2019 stated “Naloxone is a prescription-only medicine, so pharmacies cannot sell it over the counter” however goes on to state, “drug services can supply it without a prescription. And anyone can use it to save a life in an emergency” and under regulations that came into force in October 2015, people working in or for drug treatment services can, as part of their role, supply naloxone to others.
It was this change in legislation in 2015 which opened the door to enabling those with Lived and Living Experiences of drug use to begin to make supplies of Naloxone to their peers providing they were attached to “a drug treatment service” or working in a volunteer capacity.
It should be noted that pre-2015 many drug user activists across the UK were supplying Naloxone to their peers as part of clandestine user-led harm reduction projects. To all these guys I salute you!!
Remember earlier when I said people who use drugs should know their place, well the 2015 legislation allows them to do just that. To work at the coal face, across communities using their privileged access and authentic skills to actively reduce the number of drug related deaths across the UK by supplying Naloxone.
Building Peer to Peer Naloxone Training and supply programs
So how do you go about widening the supply of Naloxone? Well one such way is by training and supporting those with lived and living experiences of addiction to go out into their communities, to tap into their networks and train and make supplies of Naloxone to their peers. This is what is known as the Peer-to-Peer approach and its awesome and not complicated to develop and implement.
In October 2020 the Office of National Statistics released its data pertaining to Drug Related Deaths and to no surprise (however with great sadness) we have seen another annual rise across England and Wales in 2019 seeing 4,393 tragic, needless and avoidable deaths, At least 15 people die of a needless and avoidable drug related death each day in the UK and we know that over half of all deaths involved an opiate meaning that if we had wider access to Naloxone, without doubt, many lives could have been saved.
According to the European Monitoring System for Drugs and Drug Addiction (EMCDDA), “Many of those who die from opioid overdose are not alone at the time of death, suggesting that an early intervention, such as the administration of naloxone, can prevent opioid-induced deaths”. The idea behind getting Naloxone into the hands of people who use opioids is arguably ‘no brainer’ as ‘they’ according to World Health Organisation: ‘have a 50-70 % lifetime risk of having an overdose and also because they are more than likely to be a bystander or present at an overdose’ (WHO, 2014).
I hope by now I have convinced you that widening the supply of Naloxone is a win win for all concerned, coupled with the fact that everything from a legislative perspective now allows for people with lived & living experiences to train and supply Naloxone to their pals then all that’s left is to tell you how I did it.
So in a nut shell the P2P Naloxone projects I have been developing with providers across the UK encompasses 3 key areas, all of which are completed across a period of 12 weeks. The basic training model comprises of:
Month One: Community mobilisation & Tech Support: The starting point is where I work with providers and whole staff teams to outline the model for P2P supply ensuring that everyone is on board and ready to receive the project. It is important that providers and staff recognise that this project is not a ‘recovery project’ but rather a ‘harm reduction project’ and as such the people best placed to go out into the community to make supplies of naloxone are existing drug users from the local community or perhaps even current clients who are in treatment with the hosts organisation.

I have heard it said in the past that people need to have ‘X’ amount of “clean time” (a statement I hate) before you are able to volunteer with a given service which I feel sadly discriminates against a group of individuals who are best placed to make P2P projects like this a real success. Release in their (2019) Saving Lives report suggest,
“Empowering people who use (or have used) opioids to supply, carry and administer naloxone can significantly improve access for those who might experience an opioid overdose, thereby saving lives. People who use (or have used) opioids are experts by experience; their use of anecdotal evidence in naloxone supply/training provides added credibility, authenticity and effectiveness whilst simultaneously debunking myths about overdoses"
It is so important right at the start of the Peer-to-Peer projects that you develop that you recognise the unique and authentic skill set that people who use drugs possess and welcome them into this work and your services with open arms as equal partners, they will make the project great I promise.

Also during the first month I spend time on the ground meeting the wonderful clients of services and also those who are treatment naive to tell them we need their support and involvement to build and co-produce these projects. Lots of time is spend building positive rapports and relationships with these guys so they know that we are sincere in our ask for their support. Remember these guys have been knocked back time and time again in the past, so whilst your ask for support may come as a bit of a shock to them or be met with a little distrust initially, don’t worry, you won’t have to sell the project too hard, these guys want to stop their pals dying, they will be all in for sure.
Month two: Product familiarisation: So once you have worked with the provider and ironed out any sticking points such as paying volunteer expenses (that's what these guys are, and defiantly not free labour) you are now ready to begin to work with the guys and girls you have recruited to the project and get started with the product familiarisation process where they will get their hands on Naloxone and begin to learn their trade.
It really is a beautiful thing to be part of man, to see the guys get really excited, to listen to the authenticity of what they do, each of them with their own unique but expert way of doing things!!

Be prepared to start seeing a master class unfolding in front of your eyes, in fact be prepared for your Naloxone Champions to begin to teach you, because these guys just get it, and for many of them you can be sure, that this will not be the first time they have got their hands on Naloxone, many of them will have already saved the life of someone they know with Naloxone. These guys are Hero’s, all of them!!
We practice and rehearse using the Naloxone Checklist, We have first aid training and Basic Life Support training, we plan for where we will supply Naloxone out in the community and we drink copious amounts of tea and coffee and eat loads and loads of biscuits (which are an essential part of any peer to peer project).
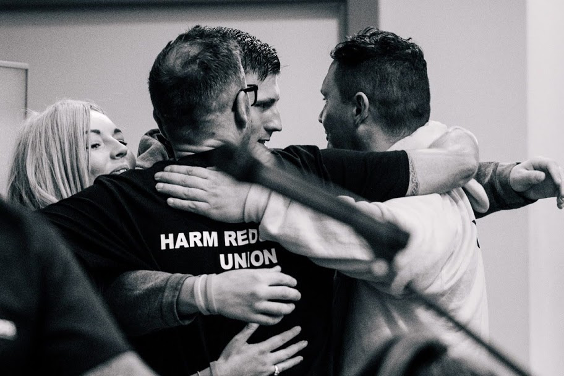
We get given hoodies with Naloxone Champion, "Ask me about naloxone” written on them, and there are no words to describe how you make us feel when you do this... We have arrived, and we feel proud of ourselves, perhaps for the first time in decades that we have felt this way. Someone believes in us and we won’t let you down, just watch!!

We share stories about addiction, about life, about the devastating loss of friends as a result of drug related deaths, we become close and “Part of” something truly beautiful. Oh and at times we laugh, we laugh so hard that we cry. We may have just found the very thing that makes us feel like we are special, like we are not just scum and a drain on society, but instead people capable of saving lives whilst being backed and supported by providers who truly believe in us and our abilities, the magic is happening, and we love it.
Month three: Bringing it all together and hitting the streets: And finally, we are almost there, we have spent a month meeting on a regular basis, tightening up our skills, planning where people who use drugs go and how we will make our offer of Naloxone to the people we meet on the streets. We talk about what we will do if we are challenged by a member of the public when making supplies, which incidentally we never have been, people love what we do, oh and we don’t worry about the police and what they will say, as they have been involved from the outset. In fact, on every project I have developed, police have played a significant role in the success of all of these projects. They too don’t want people to die of needless and avoidable drug related deaths either, so we always have their backing and their support for which we are truly grateful.
So finally we fill backpacks with all the things we need to make supplies, obviously the Naloxone and loads of it (these guys are going to supply loads of kits). We carry copies of the Naloxone Checklist so we can ensure uniformity of messaging when training and making supplies, we carry wrist bands which say “I carry take home Naloxone” which we give to every person we supply a kit to, and lastly not something that we put into the bag but instead carried in the hearts of each of the peers is the desperate desire to reduce drug related deaths at all costs.
Seeing the Naloxone Champions I work with hitting the streets for the first time and making supplies of Naloxone to their pals gives me goose bumps, in fact as I type this right now, my body is covered in them. I cannot express the pride and admiration I have for each of them. I listen to them make that first supply, the message is on point, the connection with the person they are training is instant, I witness something very special indeed, something which I find hard to put into words, it is magical to see and even more magical to be part of. I am blessed to be part of their journeys.

They hit the streets, the back lanes, disused carparks, they go to the places where drug users go. The connect instantly, they command the moment, they deliver impeccable overdose awareness training in the place where they stand, they demo the kit, their training skills are indescribable however always professional and it’s done, a sealed kit of Naloxone is handed over, along with a wrist band and a tear off sheet to remind their pals of what they have just been taught, and then with pride and a spring in their steps they are off to seek out the next person to train, who like the person before them will be able to save a life after a brief encounter with the awesome Naloxone Peers.

This training and supply process is beautifully simple but so astronomically powerful to see happen. It’s a privilege to see these guys grow and change from people who didn’t believe in themselves 12 weeks earlier to a group of people who now feel on top of the world and in their rightful place, one which allows them to save the lives of their pals through making supplies of life saving naloxone.
Some key lessons I have learned from building projects like this:
As I begin to bring this longest blog ever to a close, I just want to point out some brief but important lessons I have learned thus far:
1.Having direct access to executives & decision makers is crucial in formulating plans and driving the project forward:
This is really important as we want to develop these projects in quick time so having a direct line to decision makers means we are not waiting weeks and months to get something agreed. This is also why the technical support element at the front of the program is so important as it allows us to identify and address any worries or concerns right from the word go.
2. There needs to be access to sufficient naloxone to meet the demand of P2PN:
It is crucial that you have adequate supplies of Naloxone as when the peers start their work the number of kits being supplied is going to rise significantly. Ensure you protect budgets to enable enough Naloxone to be purchased. This work saves lives!!
3. Use the unique skills and local awareness of people who use drugs – they have privileged access to hidden populations and are authentic and credible in their approach:
Ensure you truly believe in people who use drugs and their ability to co-produce and create projects with you, just because someone uses drugs does not mean that they won't deliver first class interventions for you. People who use drugs and those with lived and living experiences are the best people for the job for sure, you never know you may find you even learn loads from working with these guys.
4. Drug user groups and peer initiatives need to be autonomous from providers, so they are sustained regardless of changes in provider:
Protect P2P projects like this at all cost, give peers ownership of the project to ensure that if you lose your contract, that the great project you have developed with the peers does not end just because a contract does. P2P supply should be led and driven by peers and should continue regardless of which provider holds a contract in a given area.
5. P2PN is part of wider toolkit of interventions for people who inject drugs and are at risk from opioid overdose:
When you have built your awesome P2P Naloxone projects, don’t just see that as the end point. Learn from your experiences and the experiences of the peers. See their worth and their value and work with them to explore next steps for new peer driven projects. I’m not going to tell you what these are because I’m gonna build them with peers and providers in the weeks and months ahead, however watch this space because more awesome projects are coming ha-ha!
6. Be prepared to move quickly and I mean quickly:
When you work with people who use drugs on projects like this, the pace will be rapid. Don’t be intimidated or paralysed by this, get on board, trust in the process and watch the magic happen.
So the last thing I want to say to you all...
I never believed when I set out to develop this project that it would transform my own life in the way that it has. I’ve been blessed to have been able to work with some of the most inspiring people I have ever met. We start out these projects as strangers and over the weeks and months that follow, we become friends. That’s right, not seeing me being close to “clients” in my role as a “professional” but me having love for these guys as friends because that’s exactly what they are, my friends!!
So to all the wonderful Naloxone Champions I have worked with over the past 18 months I want to say thank you, thank you for your belief in me and in these projects. I am humbled always by your courage and your commitment and in awe always of who each of you are as individuals, I love you guys!!
And to the forward thinking providers who also agreed to build these projects I also extend a huge thanks and debt of gratitude to you too. You opened your minds and your hearts to these projects, your actions have saved many lives and not just that of people who are overdosing daily in our communities, but also the lives of the peers who would tell you that allowing them to be part of projects like this have saved their lives too. On behalf of all of them thank you!
And lastly to you the reader ….
I hope one day soon you to get to feel the magic as I do from developing projects like this. For me it has been the most important development project I have ever worked on and I really hope you feel inspired to build your own P2P Naloxone Training & Supply projects. As I write this last sentence, again I am covered in goosebumps, I’m sat with a smile on my face and a heart beaming with pride because this is what it means to us - Thank you!!
George Charlton works as an independent trainer and consultant across the UK developing innovative and dynamic projects which put people who use drugs and those with lived and living experiences of addiction front and centre. For more information about his work please email info@georgecharlton.com
References:
https://www.emcdda.europa.eu/system/files/publications/2089/TDXD15020ENN.pdf
EMCDDA (2016), Preventing opioid overdose deaths with take-home naloxone, Publications Office of the European Union, Luxembourg.
https://www.euronpud.net/naloxone
World Health Organization (2014), Community management of opioid overdose, World Health Organization, Geneva.